
Our slides:
http://docs.google.com/presentation/d/19iVJI2LxgB2jzGHOwYtLk6T2JeJJYuVE3eteym2441o/edit?usp=sharing
Our slides:
http://docs.google.com/presentation/d/19iVJI2LxgB2jzGHOwYtLk6T2JeJJYuVE3eteym2441o/edit?usp=sharing
Our biggest hurdle is to figure out if we want to make a matt or a shoe, but to do that, we first need to remind ourselves how to use Arduino! We also spent a bit of time figuring out what to tackle in what order, and imagining what materials we will need throughout the process.
To refresh our memory, we did some labs from the P-Comp website. The FSR lab was a success– allowing Arduino to play tones base on the tone library. The MIDI lab was a different story- We couldn’t get the computer to recognize the midi interface. ![]() We will need help with this one.
We will need help with this one.
http://www.youtube.com/watch?feature=player_embedded&v=-NwtG4GwsrQ
Here’s an image of our setup. We tried moving a few things around with no success.
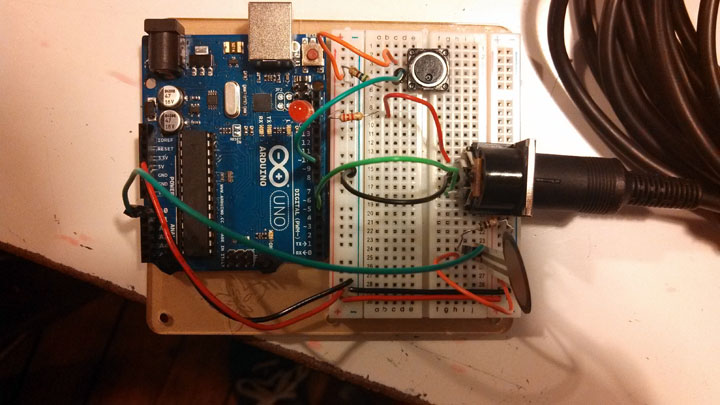

We were able to get the LED to light up but no power seemed to go to the MIDI box. When we opened up garage band, the program said that it didn’t detect any MIDI inputs.
http://www.me-ality.com/
http://www.jazzasmovement.com/wheres-the-beat.html
http://itp.nyu.edu/~mam1286/milazzo_ma/?p=206
Reading “The effect of a new syringe design on the ability of rheumatoid arthritis patients to inject a biological medication” provided me with some valuable insights into the process of testing a new design. The fact that this was done in an academic journal makes sense because it is a product designed specifically for the medical field, a decidedly academic field, HMO’s aside. I’m curious, though how ergonomic designs for less-academic realms are tested though, and if they are put through the same scientific rigor as this one. I didn’t detect many limitations besides those noted by the researchers, and they clearly disclosed their biases as employees of the company funding the study. Those things aside, the new design is clearly an improvement over the old one, improving the leverage of the patient, and their overall ability to use the product for its intended purpose. Aesthetically and functionally, improvement has been made through this design.
Though improvements are significant, they are not dramatic or surprising, and it is apparent to me that the designers are working within an old paradigm. The highest ratings and some of the biggest overall improvements for the new design were in aesthetic areas, which may indicate that the look of the product had a more significant role in the overall improvement in use of the product than increased functionality. When comparing the the images of patients using the new and old products, there is almost no difference. Both patients have bent wrists, compromising the ability of the hands to do work. It seems that any design aimed at improving hand functions should first look at the wrist position that it requires of users, considering that all muscles controlling the hand travel through the carpal tunnel. Putting the wrist in the best possible position would likely require a more significant re-design than that of this study, but would likely provide more dramatic improvements. Of course, I am not a medical professional, so there may be other aspects of the problem that I am missing.
Original post with images: http://itp.nyu.edu/~mam1286/milazzo_ma/?p=194
For week two of Biomechanics for Interactive design, I mapped the range of motion of the ankle joint in the Sagittal plane. This about.com article notes that the plantar flexion(downward movement) is 50 degrees and the dorsiflexion(upward movement) is 20 degrees. I also found a very helpful animated video that explains the anatomy and movement of the ankle. After my initial research I did some sketches.
The first few explored the anatomy I had learned and tried to apply it to movement in the Sagittal plane. My first idea for mapping the range of motion, seen in the middle row on the right side, was to create a pulley system that would replicate the pulling of the Achilles and Anterior-Tibial tendons on the ankle bones to create movement. Due to time constraints and limited resources, though, I decided to take on a different approach. I created a model of the joint with limited movement range, simulated by physically blocking movement close to the 20 degree dorsiflexion and 50 degree plantar flexion.
http://itp.nyu.edu/~mam1286/milazzo_ma/?p=177