I met Pinky Magbanuaan occupational therapist in NYC, last Friday and we had a elabrote discussion about CTS and my project idea.
I also read few articles and papers on the syndrome and current generally accepted treatments and precautionary measures in the area.
Human hand anatomy . The human hand facilitates flexion-extension, and radial and ulnar deviation. This is achieved by an intricate mechanism of movement of anatomical structures (bones, tendons and ligaments). The human hand has 27 bones, of which 8 bones are carpal bones, 5 bones are metacarpal bones and the remaining 14 bones are digital bones (proximal, intermediate and distal phalanges). The carpal tunnel is a channel formed by eight carpal bones of the wrist covered by a tough ligament called the flexor retinaculum. This channel contains nine tendons and the median nerve. The median nerve supplies sensation to the thumb, index finger, middle finger, and half of the ring finger. Insufficient space in the carpal canal can cause a direct pressure on the median nerve in the event of change in the volume due to inflammation or fluid retention. The little finger and the other half of the ring finger have sensation supplied by the ulnar nerve, which does not travel through the carpal tunnel.


Turning the palm down is called PRONATION
This is also a forearm motion, not a wrist motion. The name can be remembered because this is the position to POUR soup out of your hand.

Turning the palm up is called SUPINATION.
This is a forearm motion, not a wrist motion. The name can be remembered because this is the position to hold SOUP in your hand.
Wrist Motions : Flexion and extension/Radial and ulnar deviation.

What is wrist flexion and extension?
Wrist extension is the upward movement of the wrist to which results in the palm facing outward, while wrist flexion is the downward or inward movement of the wrist which results in the palm facing inward (see illustration below). Both movements reduce available strength, however flexion can cause up to 55% reduction in strength at just 25° of motion from a neutral position.

What is wrist radial and ulnar deviation?
Radial and ulnar deviation is the side-to-side movement of the hand at the wrist, toward or away from the thumb. Radial deviation causes up to a 20% reduction in hand strength with just 25 ° of motion from a neutral position. At 40% Ulnar deviation a similar drop in available strength is observed (see illustration).
About the syndrome: Compression of the median nerve at the wrist is the most common upper extremity compression neuropathy.

Recent data indicates that CTS may affect approx. 0.1% of the population of US of A per year*.
(Tanaka S, et al: The US prevalence of the self-reported carpal tunnel syndrome:1988 national health review data, Am J Pub Health 84: 1846, 1994.)
The bureau of Labour Statics has estimated that 1997, there were 29,200 cases of CTS that required time of from work*.
(American Academy of Orthopedic Surgery Bulletin, April 2000, p.5)
There are three different nerves which exit the cervical spine, penetrate under the clavicle (Collar bone,) continue into the armpit and into the shoulders, forearms and hands. The nerves are: The Median n, the Ulnar n. and the Radial n.

The carpal tunnel is an anatomical compartment located at the base of the palm. Nine flexor tendons and the median nerve pass through the carpal tunnel that is surrounded on three sides by the carpal bones that form an arch.

The median nerve provides feeling or sensation to the thumb, index finger, long finger, and half of the ring finger. At the level of the wrist, the median nerve supplies the muscles at the base of the thumb that allow it to abduct, or move away from the fingers, out of the plane of the palm. The carpal tunnel is located at the middle third of the base of the palm, bounded by the bony prominence of the scaphoid tubercle and trapezium at the base of the thumb, and the hamate hook that can be palpated along the axis of the ring finger. This tunnel is normally narrow, so any swelling can pinch the nerve and cause pain, numbness, tingling or weakness. This is called carpal tunnel syndrome.
Pathogenesis:
The cause of CTS may be divided into three general areas:
- The anatomy of the carpal tunnel proper, both systemic and local
- Pathophysiologic disorders
- CTS related to functional use
Some people who develop this problem were born with a carpal tunnel that is small. Many people believe that carpal tunnel syndrome is caused by making the same hand and wrist motion over and over. In fact, using hand tools that vibrate may lead to carpal tunnel.
Treatment
Generally accepted treatments include: steroids either orally or injected locally, splinting, and surgical release of the transverse carpal ligament. There is no or insufficient evidence for ultrasound, yoga, lasers, B6, and exercise therapy.
Clinical Practice Guideline on the Treatment of Carpal Tunnel Syndrome. American Academy of Orthopaedic Surgeons. September 2008.
Piazzini, DB; Aprile, I; Ferrara, PE; Bertolini, C; Tonali, P; Maggi, L; Rabini, A; Piantelli, S; Padua, L (2007 Apr). “A systematic review of conservative treatment of carpal tunnel syndrome.”.Clinical rehabilitation 21 (4): 299–314. PMID 17613571.
http://udini.proquest.com/view/design-development-and-validation-pqid:2299974251/
Diagnosis:
A combination of described symptoms, clinical findings, and electrophysiological testing is used by a majority of hand surgeons. A predominance of pain rather than numbness is unlikely to be caused by carpal tunnel syndrome no matter what the result of electrophysiological testing.Electrodiagnostic testing (electromyography and nerve conduction velocity) can objectively verify the median nerve dysfunction. If these tests are normal, carpal tunnel syndrome is either absent or very, very mild.An electromyogram (EMG) measures the electrical activity of muscles at rest and during contraction. Nerve conduction studies measure how well and how fast the nerves can send electrical signals.Nerves control the muscles in the body with electrical signals called impulses. These impulses make the muscles react in specific ways. Nerve and muscle problems cause the muscles to react in abnormal ways.
NCV:
EMG test that uses fine electrode needles inserted through the skin into the muscle, a nerve conduction study uses surface patch electrodes (similar to the ones used for an EKG/ECG of the heart).These sticky electrodes are placed over the muscles and nerves that are being tested. The nerve is electrically stimulated (Doctor talk for a little shock-like sensation) by the frist electrode (furtherest up the arm) while a second electrode detects the electrical impulse “down stream” from the first.The resulting electrical activity is recorded by the other electrodes. The distance between electrodes and the time it takes to travel between electrodes are used to calculate the speed of the impulses and is reported out as milliseconds.
Related projects:

Neri Oximan: Wrist Splint
Carpal Skin is a prototype for a protective glove to protect against Carpal Tunnel Syndrome. Carpal Skin is a process by which to map the pain-profile of a particular patient—its intensity and duration—and to distribute hard and soft materials to fit the patient’s anatomical and physiological requirements, limiting movement in a customized fashion. The form-generation process is inspired by animal coating patterns in the control of stiffness variation.
Neri Oxman’s research focuses on the inspiration of Nature, particularly biomimicry on digital design and fabrication technologies. Biomimicry examines models, systems, processes and systems of nature with the aim of taking inspiration from nature to solve human problems such as illness (but also human dwellings, etc. Indeed, logic, behavior of natural systems can be shifted into built environment, as her research demonstrates). Biomimicry and biology inspire her design and fabrication method.
The Carpal skin acts to demonstrate the notion of a structural skin using pattern, here the animal coating.
http://web.media.mit.edu/~neri/site/projects/carpalskin/carpalskin.html
My area of study:
Wrist/muscle motion that effects /causes carpal tunnel:
Repetitive motion involving the wrist in flexion, extension and ulnar deviation, as well as digital flexion and extension may cause CTS*.
(Possible role of carpal hyperextension in superficial digital flexor tendinopathy.:
http://www.ncbi.nlm.nih.gov/pubmed/21880065)
(Reference book: Rehabilitation of the hand and upper extremity by Mackin, Callahan Skirven, Schneider & Osterman, volume 1 fifth edition.)
Splinting of wrist is the initial care to treat mild CTS. Traditional cock-up splint and commercially available splints place the wrist in the functional position of 20 to 30 degrees of extension. Many scientific studies show that carpal canal pressure increases with increasing wrist flexion and extension. In 1995, Weiss et al demonstrated that the slowest pressure in the carpal canal was when the wrist was positioned in 2 degree(+- 9 degrees ) of flexion and 1 degree(+_9 degree) of ulnar deviation for patients with CTS.
Many health professionals suggest that, for best results, one should wear braces at night and, if possible, during the activity primarily causing stress on the wrists.
Wrist posture during computer pointing device use.: http://www.ncbi.nlm.nih.gov/pubmed/10619116
My proposal:
My study didn’t show any pre existing device which alerts user of there prolonged wrist flexion, extension and ulnar deviation in a particular degree.
Though a lot of study have been done on mouse designs on wrist posture to come up with ergonomically designed computer mouse. (http://ergo.human.cornell.edu/pub/hflabreports/mouserep.pdf)
Wrist movements in flexion-extension and radial-ulnar deviation are coupled. Maximal wrist range of motion is near the neutral position. To account for the naturally coupled wrist motion in work station design and rehabilitation, the wrist should be placed at a neutral position.
http://www.ncbi.nlm.nih.gov/pubmed/15621323
http://www.vistalab.com/commoninjuries.asp
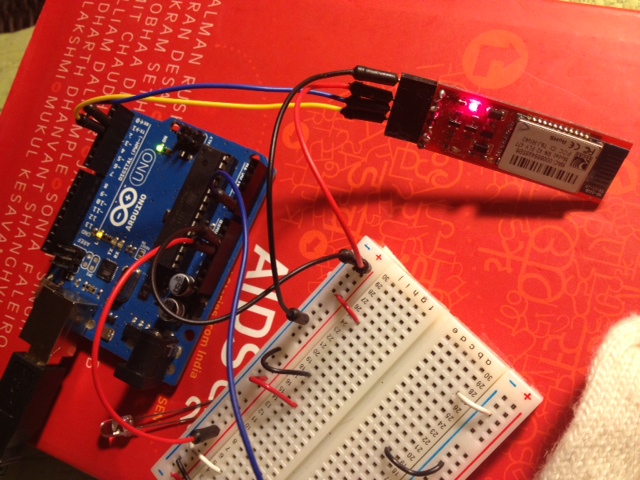
First step: My device will monitor wrist movement and time spend in particular degree of flexion-extension or radial-ulnar deviation with visualization and sensors/actuators (Electroactive Polymers) will help to change the motion and alert the user of the wrist movements. I am also thinking of integrating nerve conduction velocity test to make an alarm system.









{kind=link}